What TMS can and cannot do for dementia
TMS is not a cure for Alzheimer’s or any other dementia. It does not clear away the proteins behind the disease. It does not reverse damage that has already happened, and it cannot bring back memories or abilities that are already gone. Any clinic that tells you otherwise is not being straight with you.
What the research does suggest is smaller and more realistic. In some people with mild to moderate Alzheimer’s, certain TMS protocols may slow how fast cognition and daily function decline over a course of treatment. TMS may also help with symptoms that often travel with dementia, especially depression, low mood, and apathy. Those are real goals. They are not the same as a cure.
What is happening in the brain with Alzheimer's and MCI
Alzheimer’s is driven by changes in the brain, the buildup of amyloid and tau proteins, that damage and disconnect neurons over time. But the symptoms people notice early on are also a story about brain networks losing their connections.
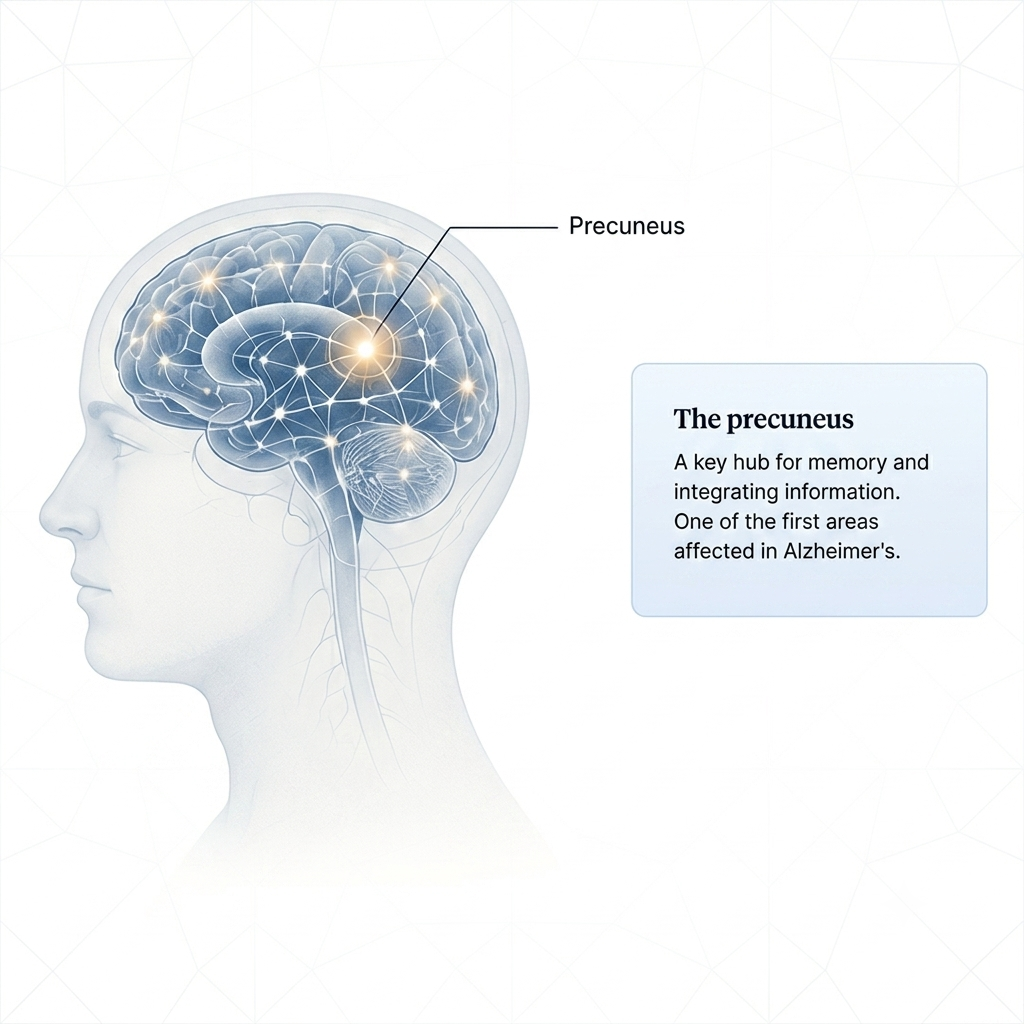
One of the first regions affected is a hub called the precuneus. It sits at the center of the network the brain uses for memory and for pulling information together. As Alzheimer’s moves forward, the precuneus and the circuits tied to it have a harder time communicating. The brain’s ability to form and strengthen connections, called plasticity, drops off.
TMS does not change the proteins behind the disease. It works on a different layer: the activity and connectivity of the brain circuits that are still working. Focused magnetic pulses are used to raise activity and strengthen connections in those circuits while they are still healthy enough to respond. This is also why timing matters in the research. Earlier in the disease, there is more for TMS to work with.
We don't ask you to trust us. We show you the research.
The precuneus protocol, the most promising recent data
The largest review to date
The most-studied target, and the faster version of TMS
Where the FDA stands
A one-day approach, and why that matters for caregivers
For an older adult with memory loss, the schedule is often the hardest part. Daily clinic visits for weeks, then ongoing upkeep, can be a lot when a patient depends on a spouse or an adult child for every ride. A treatment that isn’t realistic is a treatment that doesn’t help.
Closing that gap is the whole idea behind our One-Day Intensive, and the early research is starting to point the same way. A 2024 case report tested a single-day protocol in Alzheimer’s patients. Each treatment day paired a dose of D-cycloserine, a medication that boosts neuroplasticity, with a series of short iTBS sessions aimed at the precuneus, repeated just once a month for five months. Both patients, ages 78 and 83 and new to TMS, improved on standard memory and thinking tests, and the gains mostly held across the follow-up months. It is the same set of ideas behind our accelerated work. Shorten the schedule, add a medication that helps the brain change, and make treatment something families can actually do.

Read this as a signal, not a promise.
This was two patients, with no comparison group and no placebo. That is the weakest kind of evidence. It cannot tell us how much of the change came from the treatment versus chance or normal ups and downs. We share it because it suggests a faster, caregiver-friendly approach may be workable and worth studying, not because it proves the approach works. The authors say controlled trials are needed. We agree.

Want to talk through whether a one-day approach fits?
There is no one-size-fits-all approach to dementia treatment, but that doesn’t mean there’s no hope. What we can do is sit down with you, look at the diagnosis and the stage, walk through what the research does and does not support, and tell you honestly whether an accelerated approach is worth considering for your family.
Curious how a full course of TMS fits into a single clinic day? See how our One-Day Intensive works.
Where TMS may help?
Memory and thinking (slowing the slide)
Mood and behavior (firmer ground)
Is TMS worth a conversation for your situation?
It may be worth talking about if:
- You or a loved one has mild cognitive impairment or mild to moderate Alzheimer's. These earlier stages have the strongest evidence.
- You want something to add to current care, not a replacement for medication or other treatment.
- Depression, apathy, or low mood are part of the picture.
- You understand this is an investigational use and want an honest read on whether it could help.
- The patient can sit for treatment sessions and follow simple instructions.
- The patient has advanced dementia. The current evidence does not support a benefit at that stage.
- There is metal in or near the head, a history of seizures or epilepsy, or certain other neurological risks.
- You are looking for a cure, or expecting lost abilities to come back.
- The patient cannot tolerate the treatment setting.
Note: A licensed clinician decides eligibility after a full review. The consultation is where we figure out, honestly, whether this makes sense for your family.
What treatment looks like?


Is TMS safe for older adults?
TMS has a strong safety record across more than twenty years of use, including in older adults. The most common side effects are mild scalp discomfort or a short headache around the time of a session, and they usually pass. There are none of the body-wide drug effects that medications can bring, no sedation, no weight gain, no drug interactions of that kind.
The most serious risk is a seizure, which is very rare, estimated at well under 1 in 30,000 sessions. In the 143-study Mayo and Harvard review, only two studies reported any seizures at all, and most were judged unrelated to the treatment. Because seizure risk and certain neurological conditions matter more in older adults, careful screening by a clinician comes first. That is what the consultation is for.
Start with an honest conversation
OPEN NOW
Las Vegas, NV
8981 W Sahara Ave,
Suite 270
Las Vegas, NV 89117
(725) 344-3322
OPEN NOW
Springville, UT
382 E 400 S,
Suite B
Springville, UT 84663
(725) 344-3322
OPENING SOON
Conroe, TX & Casper, WY
Additional locations in development. Accelerated protocols available to traveling patients now.
Frequently Asked Question
Can TMS cure Alzheimer's or dementia?
Is TMS FDA-approved for dementia?
Does the research show TMS works?
Is the one-day approach proven for dementia?
Will Medicare or insurance cover it for dementia?
What stage is TMS most likely to help?
Is it safe for an elderly parent?
Can we do TMS alongside current medications?
Sources
- Koch G, et al. Precuneus magnetic stimulation for Alzheimer’s disease: a randomized, sham-controlled trial. Brain. 2022;145(11):3776-3786.
https://academic.oup.com/brain/article/145/11/3776/6701823
- Koch G, et al. Effects of 52 weeks of precuneus rTMS in Alzheimer’s disease patients: a randomized trial. Alzheimer’s Research and Therapy. 2025.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11963669/
- Pagali SR, et al. Efficacy and safety of TMS on cognition in mild cognitive impairment, Alzheimer disease, and related dementias: a systematic review and meta-analysis. International Psychogeriatrics. 2024;36(10):880-928.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11306417/
- Law A, et al. Single-day TMS regimens in Alzheimer’s and frontotemporal dementia: two cases (ONE-AD). Transcranial Magnetic Stimulation. 2026;7(Suppl 1):100271.
(Case series of 2 patients; preliminary and uncontrolled.)
https://doi.org/10.1016/j.transm.2026.100271
- Yang C, et al. Effects of intermittent theta-burst stimulation on cognition and glymphatic system activity in mild cognitive impairment and very mild Alzheimer’s disease: a randomized controlled trial. Journal of NeuroEngineering and Rehabilitation. 2025.
(RCT, 52 patients; cognitive gains by week 6.)
https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-025-01738-1
- NeuroAD (TMS combined with cognitive training). ALZFORUM Therapeutics database.
(FDA advisory panel: safe, but effectiveness not demonstrated; not FDA-cleared in the U.S.)
https://www.alzforum.org/therapeutics/neuroad
- Zhou Y, et al. The repetitive transcranial magnetic stimulation in Alzheimer’s disease patients with behavioral and psychological symptoms of dementia: a case report. BMC Psychiatry. 2023;23(1):354.
https://link.springer.com/article/10.1186/s12888-023-04864-z
- Cappon D, et al. Transcranial magnetic stimulation (TMS) for geriatric depression. Ageing Research Reviews. 2022;74:101531.